Get PolitiFact in your inbox.

Kevin Barrett quarantines after his former hospital roommate tested positive for COVID-19 in Seattle on Jan. 14. (AP)

The coronavirus pandemic is now stretching into its third year, a grim milestone that calls for another look at the human toll of COVID-19, and the unsteady progress in containing it.
The charts below tell various aspects of the story, from the deadly force of the disease and its disparate impact, to the signs of political polarization and the United States’ struggle to marshal an effective response.
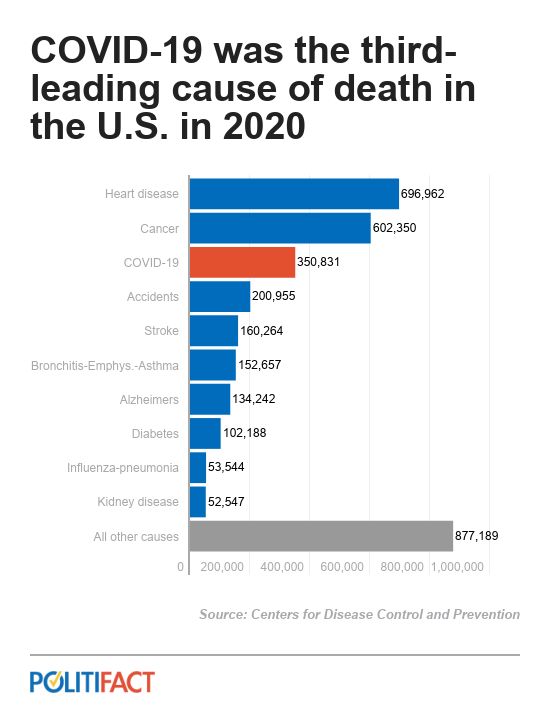
COVID-19 rocketed up the list of leading killers in the U.S. like nothing in recent memory. The closest analogue was HIV and AIDS, which ranked among the top 10 between 1990 and 1996. But even HIV/AIDS never reached higher than eighth on that list.
By contrast, COVID-19 shot up to third in 2020, its first year of existence, and that included only about nine months of the pandemic. Only heart disease and cancer killed more Americans that year.
"The leading causes of death are relatively stable over long periods of time, so this is a very striking result," said William Schaffner, a professor of preventive medicine and health policy at Vanderbilt University.
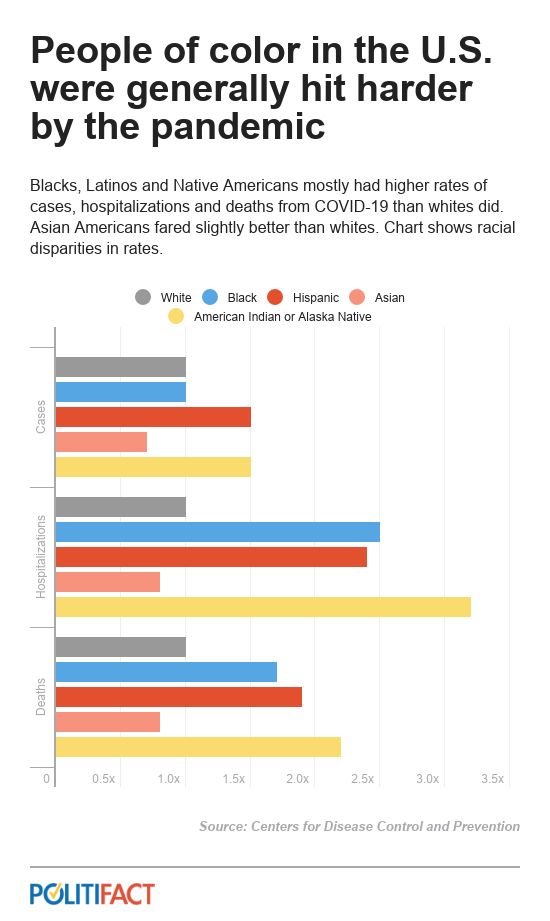
COVID-19 generally hit people of color harder, a pattern that experts trace back to historical disparities in income, geography, medical access and educational attainment.
"This tells us something about our society — it’s a kind report card," Schaffner said. Studies have shown that illness and prevention are even more strongly correlated with educational background than with income.
"There was some effort to correct the disparities," said Arthur L. Caplan, a professor of bioethics at New York University's Grossman School of Medicine. "But these were Band-Aids on a system that remains broken."
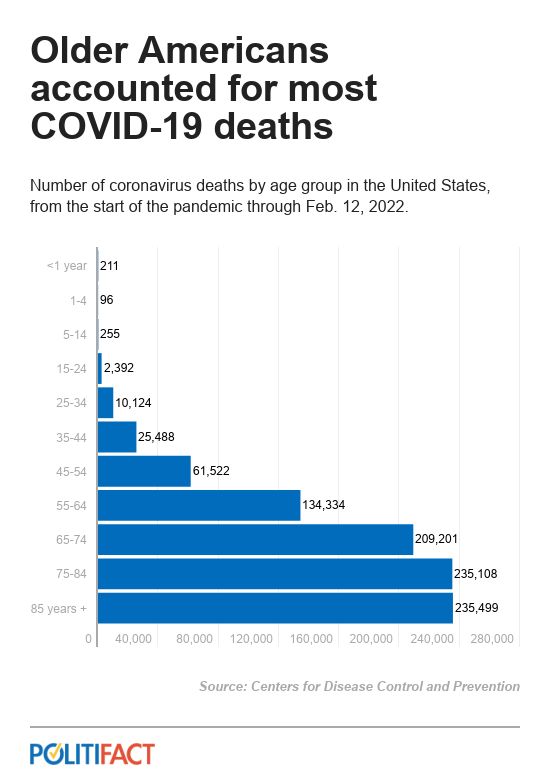
Older people tend to be more vulnerable to disease than younger people, because of weaker immune systems and underlying health problems. That’s been especially true for COVID-19.
"Many other infections affect the very young and the very old disproportionately, but COVID-19 stands out in being so age-dependent," said Monica Gandhi, a professor of medicine at the University of California-San Francisco. "Children were remarkably spared from severe disease in the U.S., as they were worldwide."
Deaths among older Americans, however, were especially widespread in the early days of the pandemic due to the close contact of senior citizens living in nursing homes.
"Some will argue that old are frail anyway, but I find that morally repugnant," Caplan said. The deaths of so many older people "makes me extremely sad."
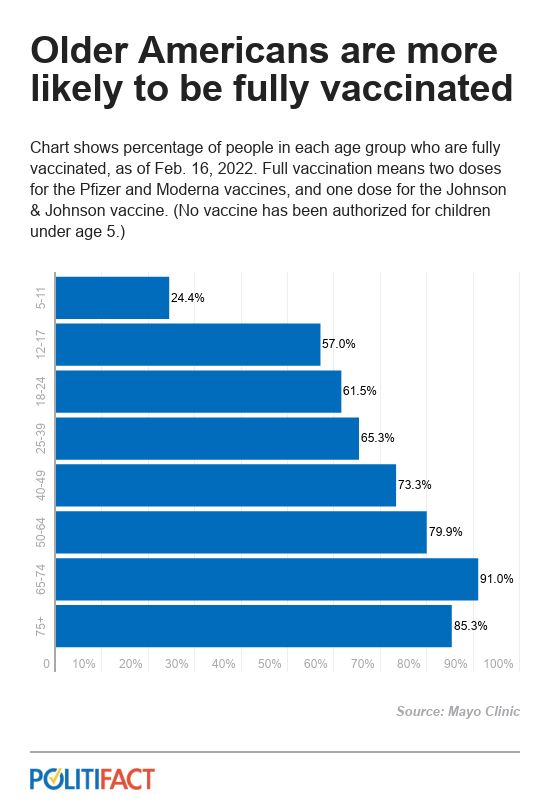
The good news, experts say, is that older Americans were the most likely to get vaccinated, with a 91% full vaccination rate for those between ages 65 and 74. This almost certainly prevented many deaths among elderly people as the pandemic ground on, Schaffner said.
The world’s performance in battling COVID-19 is analogous to the United States’: Some places did it well, and others did not.
And in the international context, the United States’ record was not so hot.
When comparing death rates around the world, it’s clear how much worse the U.S. has fared than other wealthy industrialized nations.
The countries that have a higher death rate than the U.S. are largely medium-size and middle-income. The industrialized Western nations that are the U.S.’s closest peers all managed to do better, including the United Kingdom, France, Germany, Italy and Canada.
Meanwhile, other affluent countries did far better than the U.S. did, including Japan, South Korea, and Taiwan (which have more experience with airborne diseases and greater public tolerance for masking), and two island nations: Australia and New Zealand.
In general, Schaffner said, countries that performed better than the U.S. tended to have "sustained, single-source, science-based communication. They communicated well with their populations and explained and justified why they were doing what they were doing."
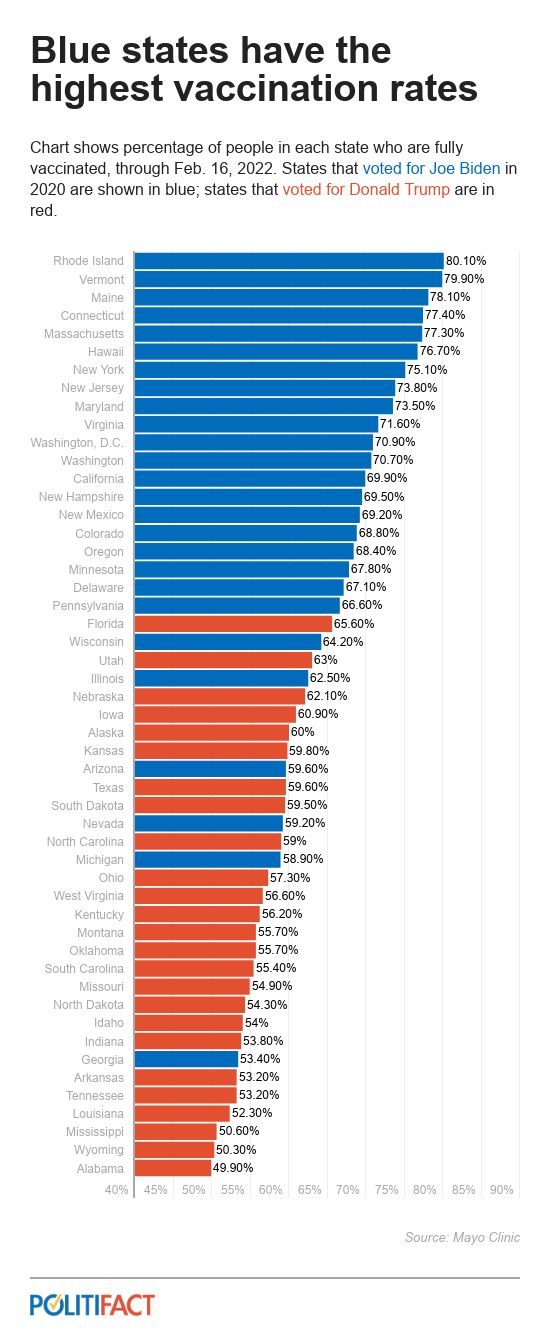
It’s impossible to look at the United States’ response to COVID-19 without factoring in the extent to which it became politicized. Almost from the beginning, basic communications about the severity of the disease and how to combat its spread broke down along partisan lines. The way Americans responded also followed a partisan pattern.
Most states that voted for Joe Biden for president in 2020 had above-average vaccination rates. Most states that voted for Donald Trump in 2020 had below-average rates.
Among the outliers in that pattern were Arizona, Nevada, Michigan and Georgia, which supported Biden but had below-average vaccination rates. All four had very tight races in 2020; and Trump won three of them in 2016. The outliers on the other side were Florida and Utah, which supported Trump but had higher-than-average vaccination rates.
Efforts to promote vaccination as advancing the common good "got beaten back by arguments about autonomy and individual freedom," Caplan said.

The rejection of vaccines by many Americans helped bring down U.S. vaccination rates compared with other countries as well.
The U.S. full-vaccination rate of just under 66% was higher than the world average of about 54%, but not especially impressive considering the United States’ wealth and the fact that it was producing many of the key vaccines in the first place. Essentially every other high-income country has vaccinated a higher share of its residents than the U.S. has.
The fact that the United States has both a lower rate of full vaccination and a higher death rate than other high-income countries "makes me wonder how we might have done as a country if our pandemic response had not been so politicized and polarized," said Brooke Nichols, an infectious-disease mathematical modeler at Boston University.
Our Sources
Centers for Disease Control and Prevention, "Leading Causes of Death, 1900-1998"
Centers for Disease Control and Prevention, "Trends in Number of COVID-19 Cases and Deaths in the US Reported to CDC, by State/Territory," Feb. 18, 2022
Centers for Disease Control and Prevention, "United States COVID-19 Cases, Deaths, and Laboratory Testing by State, Territory, and Jurisdiction," accessed Feb. 18, 2022
Centers for Disease Control and Prevention, "Number of deaths, percentage of total deaths, and age-adjusted death rates for the 10 leading causes of death in 2020," accessed Feb. 18, 2022
Centers for Disease Control and Prevention, "Provisional COVID-19 Deaths by Sex and Age," accessed Feb. 18, 2022
Centers for Disease Control and Prevention, "Risk for COVID-19 Infection, Hospitalization, and Death By Race/Ethnicity," updated Feb. 1, 2022
Johns Hopkins University, COVID-19 Dashboard, accessed Feb. 18, 2022
Johns Hopkins University, mortality analyses, accessed Feb. 18, 2022
Johns Hopkins University, worldwide vaccination rates, accessed Feb. 18, 2022
Mayo Clinic, "U.S. COVID-19 vaccine tracker: See your state’s progress," accessed Feb. 18, 2022
Kaiser Family Foundation, Median Annual Household Income, accessed Feb. 18, 2022
PolitiFact, "One year in: How does COVID-19’s toll compare with other causes of death?" Feb. 23, 2021
Email interview with Brooke Nichols, infectious-disease mathematical modeler at Boston University, Feb. 18, 2022
Email interview with Babak Javid, associate professor in the division of experimental medicine at the University of California-San Francisco. Feb. 17, 2022
Email interview with Monica Gandhi, professor of medicine at the University of California-San Francisco, Feb. 18, 2022
Interview with Arthur L. Caplan, professor of bioethics at New York University's Grossman School of Medicine, Feb. 17, 2022
Interview with William Schaffner, professor of preventive medicine and health policy at Vanderbilt University, Feb. 17, 2022